
PRP vs. Mesenchymal Stem Cells: Why Regenerative Medicine Is Moving Beyond Platelets Alone
For years, Platelet-Rich Plasma (PRP) has been one of the most commonly discussed regenerative medicine treatments in orthopedics and sports medicine. PRP helped introduce the public to the concept that the body possesses intrinsic healing mechanisms that can be concentrated and leveraged therapeutically. It was an important step forward compared to the traditional “anti-inflammatory and wait” model that dominated musculoskeletal medicine for decades.
But regenerative medicine has continued to evolve.
A recently published review in the journal Tissue Engineering and Regenerative Medicine examined the comparative effectiveness of PRP versus mesenchymal stem cells (MSCs) in orthopedic and cartilage-related applications. The emerging theme from the literature is becoming increasingly clear: while PRP can be beneficial for symptom reduction and mild tissue support, MSC-based therapies appear to offer broader regenerative potential, particularly in more advanced degenerative conditions.
At Regenezone, this is exactly why our approach has evolved into a comprehensive regenerative medicine model rather than relying solely on isolated PRP injections. Regenerative orthopedics is no longer simply about decreasing inflammation temporarily. The goal is to optimize the biologic environment surrounding damaged tissue while supporting long-term repair, recovery, and functional resilience.
PRP works primarily through concentrated growth factors derived from platelets. When injected into injured tissue, PRP can stimulate signaling pathways involved in healing, angiogenesis, collagen production, and local inflammatory modulation. In many mild tendon injuries or early arthritic conditions, patients may experience meaningful improvement in pain and function. However, PRP remains fundamentally limited by the biologic quality of the patient’s own platelets and by the relatively narrow spectrum of signaling molecules it delivers.
This becomes especially important in aging patients.
The older the patient, the more likely there is to be underlying mitochondrial dysfunction, systemic inflammation, hormonal decline, vascular insufficiency, immunosenescence, and impaired stem cell signaling. In these situations, simply concentrating aging platelets may not fully address the biologic deficits driving degeneration in the first place.
Mesenchymal stem cells operate on an entirely different biologic level.
MSCs do not merely provide growth factors. They function as highly intelligent signaling cells capable of modulating inflammation, recruiting repair pathways, supporting angiogenesis, influencing macrophage polarization, reducing fibrosis, and enhancing tissue regeneration through extensive paracrine signaling. In many ways, MSCs function more like “conductors of repair” than isolated building blocks. Much of their therapeutic power appears to come not from direct engraftment into tissue, but from their ability to orchestrate regenerative communication throughout the local environment.
This is particularly relevant in cartilage degeneration, tendon injury, ligament instability, and osteoarthritis. Cartilage possesses notoriously poor healing capacity due to limited vascularity. PRP may temporarily improve symptoms in arthritic joints by reducing inflammation and stimulating local repair pathways, but MSCs appear capable of producing a more durable biologic effect by altering the inflammatory environment itself and supporting broader regenerative activity.
The distinction becomes even more obvious clinically in moderate-to-severe degeneration.
Patients with advanced knee osteoarthritis, chronic tendon pathology, meniscal degeneration, labral pathology, or diffuse inflammatory degeneration often require a more sophisticated biologic strategy than platelets alone can provide. This is where modern regenerative medicine increasingly shifts toward MSC-based approaches, often integrated with scaffolds, extracellular vesicles, peptide therapies, hormonal optimization, rehabilitation strategies, and biomechanical correction.
The current literature increasingly reflects this trend.
Studies reviewed in the article demonstrated that MSC therapies generally showed superior outcomes compared to PRP in cartilage repair quality, tissue regeneration potential, durability of symptom improvement, and histologic tissue restoration. PRP still demonstrated benefit, particularly in milder disease states and symptom management, but MSCs consistently showed broader regenerative capabilities.
The difference can be conceptualized like this:
PRP primarily “stimulates.”
MSCs actively “coordinate regeneration.”
That distinction matters enormously.
At Regenezone, our philosophy has never been simply to inject biologics blindly into painful tissue. We emphasize a systems-based regenerative medicine approach. This includes advanced diagnostic evaluation, functional medicine assessment, hormone optimization, metabolic support, and precision ultrasound diagnostics combined with ultrasound-guided injections. Ultrasound guidance is critically important because biologic accuracy matters. Delivering regenerative products precisely into damaged ligaments, tendons, fascial planes, joints, or entheses dramatically improves procedural sophistication compared to blind injections.
We also emphasize biologic quality and sourcing.
Not all regenerative products are equal. One of the major concerns within regenerative medicine nationally is the lack of consistency in processing standards and tissue quality. At Regenezone, we utilize advanced HCT/P products sourced from FDA-cleared facilities with AATB-certified and GMP-compliant processing standards. That distinction matters for sterility, tissue integrity, safety, and biologic consistency.
Another important reality often overlooked in conventional orthopedics is that regeneration does not occur in isolation from systemic physiology.
You cannot separate joint healing from mitochondrial function.
You cannot separate tendon repair from hormone status.
You cannot separate inflammation from metabolic health.
You cannot separate biologic age from regenerative potential.
This is one reason why many patients fail conventional injection therapies repeatedly. The underlying biologic terrain has never been optimized.
Patients with insulin resistance, thyroid dysfunction, low testosterone, estrogen deficiency, chronic inflammation, endothelial dysfunction, nutrient deficiencies, or poor sleep recovery often possess impaired healing capacity before the injection even occurs. At The Hormone Zone and The Longevity Protocol, we frequently address these upstream biologic variables simultaneously in order to optimize regenerative outcomes.
Regenerative medicine is increasingly becoming integrated longevity medicine.
The future is not simply “stem cells versus PRP.”
The future is comprehensive biologic optimization.
That means combining regenerative orthopedics with hormone optimization, peptide support, mitochondrial enhancement, vascular optimization, acoustic wave therapy, rehabilitation, recovery medicine, and inflammation control into one coordinated strategy.
That is where the field is moving.
And clinically, that is where we have already been moving for years.
PRP vs MSC Regenerative Effectiveness Comparison
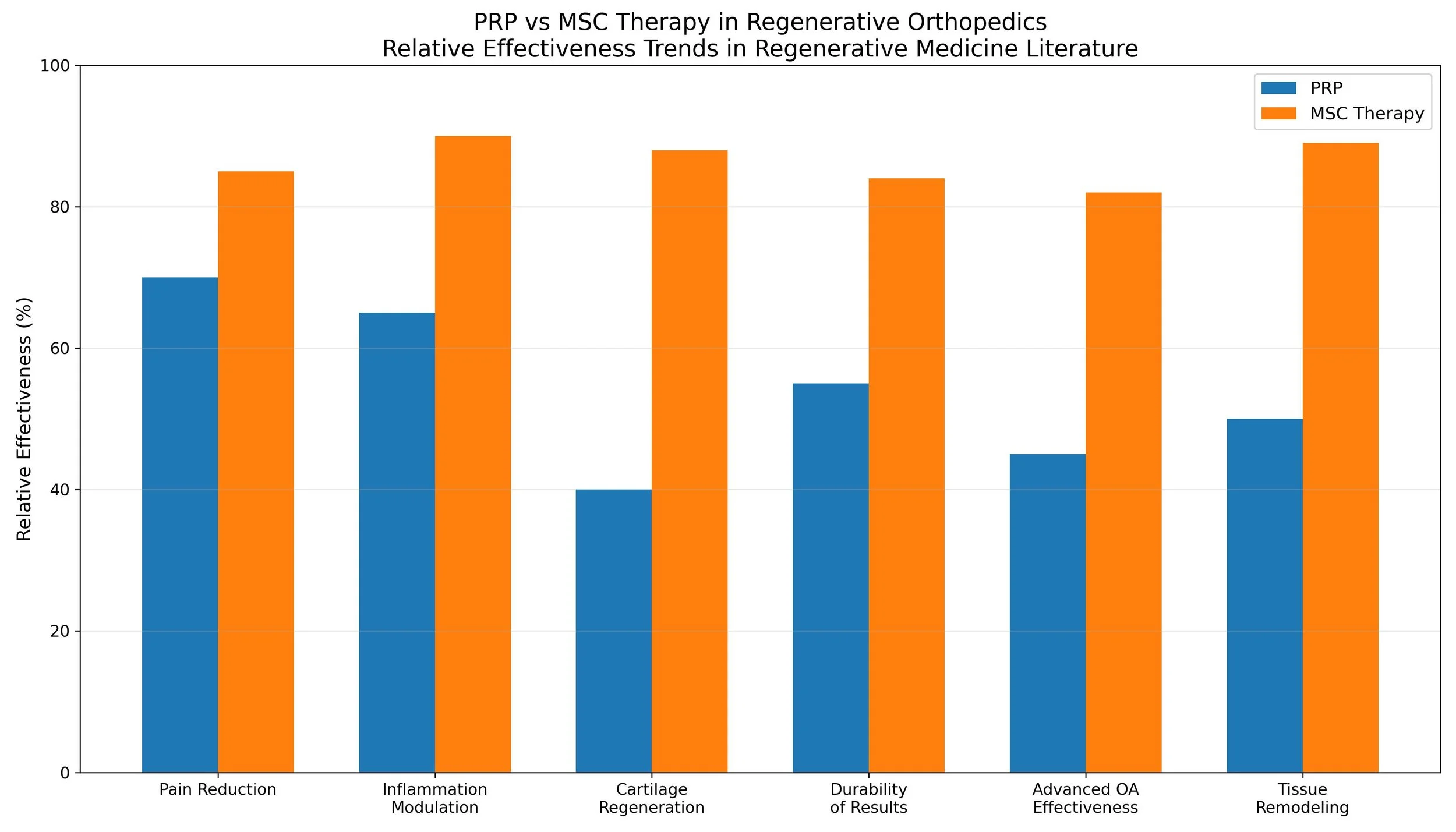
In practical clinical terms, PRP still has value. Mild tendinopathies, early arthritis, overuse injuries, and supportive recovery protocols may respond very well to platelet therapies. But for more advanced degeneration, MSC-based regenerative medicine increasingly appears to represent the next evolution of orthopedic biologic care.
The goal should never simply be symptom suppression.
The goal is restoration of function, preservation of mobility, optimization of tissue quality, and extending healthspan through biologic resilience.
That is the future of regenerative medicine.
And increasingly, the science is beginning to catch up with what many advanced regenerative physicians have already observed clinically for years.